History of Orthopaedics
The History of Casting
 Ahmed H. Abdelazeem
Ahmed H. AbdelazeemSICOT Newsletter Editorial Board Member - Cairo, Egypt
Wherever an orthopaedic surgeon is, you will hear the likes of cast, plaster and splints. Casting is an important tool in managing various types of fractures. Suffice to say that the history of casts is the history of orthopaedic practice. Its history and development are very interesting and full of stories to be told during different eras.
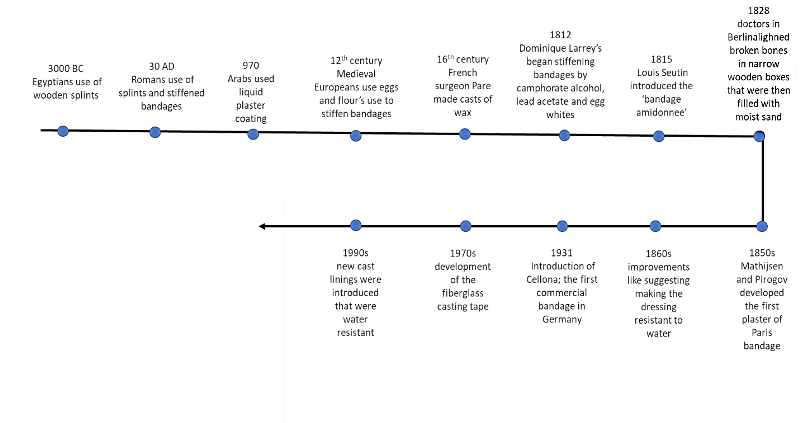
Casting and splinting have been applied for thousands of years. The first method dates as far back as 3000 BC when the ancient Egyptians used wooden splints made of bark wrapped in linen to support broken limbs. They also used stiff bandages which were probably derived from their vast knowledge of embalming techniques. Their temple walls were frequently covered in plaster of Paris but there was no evidence regarding their use in medicine. The ancient Hindus used bamboo splints for the same purpose. Later in the 30 AD, a Roman encyclopedist called Celsus, described a technique using splints and bandages stiffened with corn starch to treat fractures. In addition, ancient Greeks used waxes and resins to stiffen bandages, and lime derived from seashells and egg whites were used by Arabian doctors. In 970 AD, in his book of pharmacology, the Persian Abu Mansur Muwaffak advised that limbs with bone injuries should be coated with plaster. This technique consisted of pouring liquid plaster on the limb in a trough. In the 12th century, casts made of egg whites and flour were recommended by the Italian school of Salerno. Medieval Europeans added animal fat to the mixture. During the 16th century, the French surgeon Ambrose Pare made casts of wax, cardboard, cloth and parchment that hardened as they dried.
Interestingly, the modern cast we know can be traced back to the 19th century and has been linked with four military surgeons; Dominique Jean Larrey of France, Louis Seutin of Brussels, Antonius Mathijsen of the Netherlands and Nikolai Ivanovich Pirogov of Russia. In 1812, one of Dominique Larrey’s patients injured during the Battle of Borodino needed an arm amputation. He was immediately evacuated from Russia to France and on his arrival and removal of the bandage he had, they found that the injury had healed. Larrey concluded that the healing had been facilitated by leaving the wound undisturbed for that period. He hence began stiffening bandages by camphorate alcohol, lead acetate and egg whites. Similarly in 1815, Louis Seutin introduced the ‘bandage amidonnee’ made of wool wrap cardboard splints and bandages soaked in starch which required at least 2-3 days to dry. Velpeau, a leading French surgeon at the time also suggested the substitution of dextrin for starch which reduced the drying time to 6 hours but this was still too long especially when needed on the battlefield.
In 1828, doctors in berlin began aligning broken bones in narrow wooden boxes that were then filled with moist sand. Later quick setting gypsum plaster known as plaster of Paris was substituted for the sand. The plaster of Paris was so called because it originally came from the abundant gypsum found near Paris. It consisted of fine white powder of calcium sulphate hemihydrate which hardens after being moistened and allowed to dry. The problem with those casts at the time was that they required patients to be confined to the bed as the casts were very heavy and inconvenient.
It was Antonius Mathijsen in 1851 in Haarlem who developed the first plaster of Paris bandage. He used coarse materials like linen rubbed thoroughly by plaster of Paris, that was then moistened with a wet sponge or brush and rubbed by hand till it hardened. He claimed that this method was simple, rapid and required no assistance. He also pointed out that the bandage provided an exact fit and could be cut or windowed to provide relief when needed. Later in Russia, Nikolai Ivanovich Pirogov having observed the use of linen strips soaked in liquid plaster of Paris in sculpturing ‘Modroc technique’ and after hearing of Mathijsen’s work went on to develop his own method of plaster of Paris bandages. His method consisted of soaking coarse cloths in a plaster of Paris mixtures immediately before application and protecting the limbs with stockings or cotton pads. He used wood to reinforce large dressings.
In 1860, improvements such as making the dressing resistant to water by painting it with shellac dissolved in alcohol were introduced. Bandages continued to be made by hand in hospitals until 1931 in Germany when Cellona; the first commercial bandage was introduced.
Due to the complications of plaster of Paris bandages including skin irritation, macerations, ulceration, infection, and allergy, surgeons have tried to find other alternatives. An early plastic like material called gutta-percha obtained from latex trees was used for fracture treatment. It is hard when dry but is soft and malleable when warmed. In 1970, the fiberglass casting tape made casts lighter and more durable while also being water resistant.
Nowadays bandages of synthetic materials like knitted fiberglass impregnated with polyurethane or thermoplastic are often used. They are lighter and dry faster but cannot be molded to make a snug fit and therefore may be less comfortable. Also, plaster is smoother and does not snag clothing or abrade skin.
Cast linings are usually made of cotton but in the 1990s, new cast linings were introduced that were water resistant giving patients more freedom. However, those liners are still costly and their drying time render them somewhat inconvenient.
Waterproof covers that prevent water from reaching the cast whenever the patient is in contact with water have also been introduced. The cover is removed, dried and reused as often as necessary.
- Hernigou P. Plaster of Paris: the orthopaedic surgeon heritage. International orthopaedics. 2016 Aug 1;40(8):1767-79.