
SICOT Global Network for Electronic Learning - SIGNEL
Case of the Month
Can idiopathic pain be cancerous in children?
An 11-year-old boy presented to a clinic (outside of Prague) due to pain in the right knee which was not significant but just for check-up. The child is otherwise very fit and well.
There is no previous medical history except a history of trauma at the age of 3 which was insignificant and the parents did not bring him for medical attention until later that year. Radiographic investigations including CT scan were performed (see Figures 1-3).

Figure 1: Radiograph of both knees

Figure 2: Radiograph of both knees
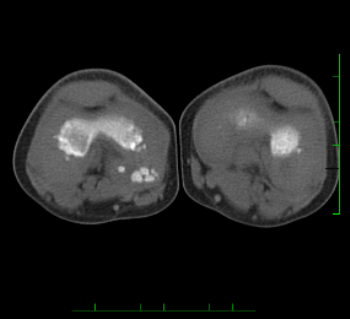
Figure 3: CT scan of both knees
Q. What would be your next step in the management of this patient?
The medical team decided to observe the patient with a regular follow-up every 6 months. However, as the child did not have any pain at all, the parents decided to self-discharge and no further review was made.
In 2016, the patient returns with a niggling type pain after sports activities. A repeat radiograph of the knee was performed (see Figure 4) and the patient was referred to our centre for further management.
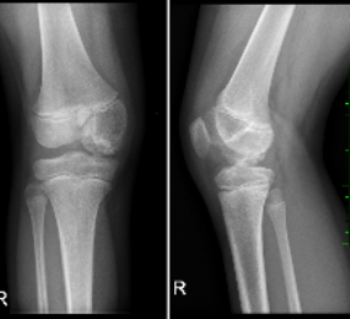
Figure 4: Radiograph of knee
Q. What is your differential diagnosis?
Osteomyelitis
Osteonecrosis
Malignant lesion
Q. What is the next step in your management?
Blood film
MRI
Diagnostic arthroscopy
Biopsy
Histology
Microbiology
Investigations that were performed are full blood tests which were completely normal including CRP and ESR. MRI scan showed chronic inflammatory process in combination with necrosis of the medial condyle of the right femur.
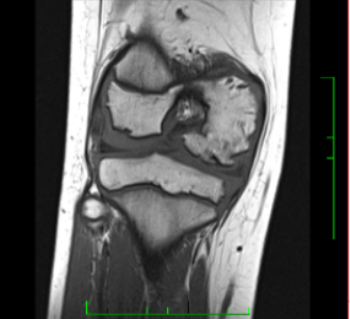
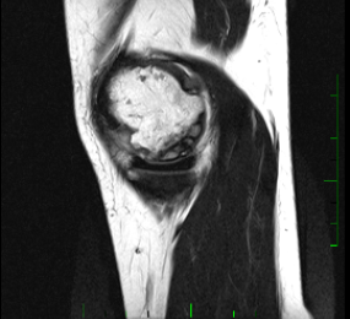
Figure 5: MRI scan of knee
Q. What is the next step in your management?
As there was no primary diagnosis at this point, a diagnostic arthroscopy and biopsy was performed.
Findings during diagnostic arthroscopy showed significant synovitis. On the medial femoral condyle, the cartilage had fragmentation and defects with nodule deformation on its lateral and caudal side. Multiple biopsies were taken. No other significant findings were noted.
Histological results showed no evidence of malignant changes. Findings were suggestive of chronic injury of the cartilage.
Microbiology results were unremarkable.
After arthroscopy and debridement, the patient was reviewed and a repeat radiograph of the knee was performed (see Figure 6).

Figure 6: Radiograph of knee
Q. What is the next step in your management?
As there was no obvious diagnosis and we failed to find what was wrong with this child, a huge question was raised: what to do next?
Q. What would be your next step?
Leave it and inform the parents that no definitive diagnosis was achieved
Repeat MRI scan
Repeat CT scan
Repeat blood tests
Repeat arthroscopic procedure
We opted to repeat the blood tests and repeat the arthroscopic procedure again. The blood tests were normal. Findings during the arthroscopic procedure showed generalised synovitis and debridement of the synovium and biopsies were taken for histology. There were signs of chondromalacia grade II / III of the medial femoral condyle. The previous biopsy sites had healed. No evidence of osteochondritis dissecans. The medial-dorsal and distal portion of femoral condyle was soft for which a micro fracture procedure was performed. No other significant findings were noted.
Microbiology and histology results were also inconclusive.
Repeat radiograph of the knee was performed at follow-up after the 2nd arthroscopic procedure (see Figure 7).

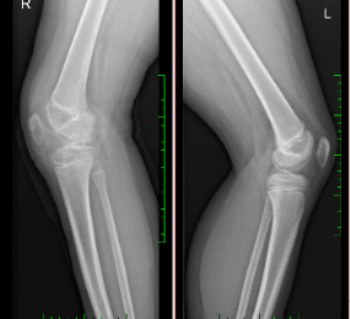
Figure 7: Radiograph of both knees
Q. What would you do now?
The child has undergone many procedures and many investigations because he was told by the initial clinic that this was most likely a tumour and he will need special attention and treatment since it is very dangerous.
There is no doubt that the initial radiograph and MRI scan were abnormal but the question that is raised is: could we have done something different? Are all the steps in our management correct?
The child and his parents still have no diagnosis and probably this case will remain a mystery as it is almost impossible to guess, after all that has been done, what the primary diagnosis is. However, there is a suggestion that the diagnosis could be osteonecrosis but without a proven aetiology and, of course, treatment plan.
- Clin Orthop Relat Res. 2013 Apr;471(4):1127-36. doi: 10.1007/s11999-012-2619-6. Osteochondritis dissecans knee histology studies have variable findings and theories of etiology. Shea KG1, Jacobs JC Jr, Carey JL, Anderson AF, Oxford JT.
- Clin Orthop Relat Res. 2013 Apr;471(4):1127-36. doi: 10.1007/s11999-012-2619-6. Osteochondritis dissecans knee histology studies have variable findings and theories of etiology. Shea KG1, Jacobs JC Jr, Carey JL, Anderson AF, Oxford JT.
- Przegl Lek. 2006;63 Suppl 7:38-41. [The pathogenesis of chrono osseous necrosis of the knee joint]. [Article in Polish] Kotela I1, Bołtuć W, Jakubowski L, Korzec A.










