
SICOT Global Network for Electronic Learning - SIGNEL
Case of the Month
History
A 15-year-old boy was hit on his right shoulder, while playing football. Physical examination showed pain, swelling and deformity of the left SC area and of the medial fourth of the clavicle. Hollow area was felt next to the right sternoclavicular joint. Neurovascular examination was normal and there was no sign of dysphagia or dyspnea.

Fig. 1: X-ray chest showing both clavicles
What is the your provisional diagnosis for this patient?
Right sternoclavicular dislocation with fracture of the medial end of clavicle.
What would be your next step in the management of this patient?
Conservative treatment
CT scan
Contrast CT scan
Surgical treatment
A Contrast CT with 3D CT reconstruction scan (Fig. 2, 3), confirmed the alignment of the floating fragment (rotated and with its medial end pointing posteriorly), which was causing compression on the right Brachiocephalic vein.

Fig. 2: Axial section from Contrast CT Scan showing compression of fracture on brachiocephalic vein
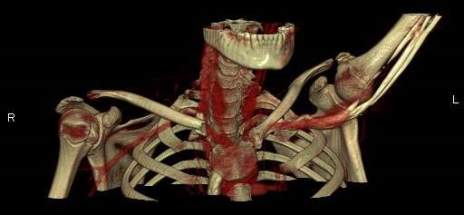
Fig. 3: Three-Dimensional Contrast CT Reconstruction

Fig. 4: Intra-operative image showing the rotated medial end of clavicle and disrupted sternoclavicular joint
The patient underwent emergency open reduction through a longitudinal incision along the medial clavicle. Surgical exploration showed the floating fragment, which was rotated and had a partially stripped periosteal sheath (Fig. 4); its medial end had a rough surface, and did not have the appearance of a cartilaginous articular surface, which corresponded to a fracture through the medial physis of the clavicle. Gentle manoeuvres were performed to reduce the fragment. Anatomic reduction and fixation of the lateral fracture with a reconstructive plate (which crossed only the lateral fracture) resulted in reduction of the fracture. Radiographic confirmation of the reduction was obtained and stability was tested with gentle mobilization of the ipsilateral upper extremity and loading of the SC joint. After surgery, the patient was placed in a sling for 4 weeks: progressive resumption of movements and activities was then allowed. After surgery the patient was asymptomatic; examination showed symmetry of the clavicles and of the SC joints, painless and complete range of motion of the left shoulder. Radiographs showed complete consolidation at three months (Fig. 5). The patient has resumed full activities and sports without problems subsequently.

Fig. 5: Three months post-operative X-ray
Discussion
Fractures and dislocations of the sternal end of the clavicle are relatively uncommon, representing less than 5% of all shoulder girdle injuries [17]. Posterior SCJ dislocations are rare, however, 30% are associated with tracheal, oesophageal or neurovascular compression, and there is a 3% to 4% mortality rate. Dislocations of the SC joint require significant direct or indirect forces, due to its strong ligamentous supporting structure [14]. The weakest link in this area in patients younger than 25 years is the SC physis, the last physis to close [6, 14]: ossification of the epiphysis does not appear on X-rays until about 18 years of age and does not unite with the metaphysis until about 23-25 years. Many so-called dislocations of the SC joint are in fact fractures through the physis (Salter-Harris I or II) [2, 14].
Association of a SC physeal fracture or SC joint dislocation with an ipsilateral fracture of the clavicle was reported in about 12 cases in the literature [1, 3, 4, 7, 8, 10-16]. Among these, cases where the clavicle fracture is adjacent to the physis [1, 4, 8, 10, 11, 14] are the most challenging, as the double injury produces a short free fragment, which is partially displaced out of the periosteal tube and rotated 90° or more [14]: this leads the sternal end of the fragment to point posteriorly and inferiorly, which exposes to risk of damage of adjacent structures (great vessels, trachea, oesophagus) [6]. In fact, similar findings have been described in our case, as in the other reported cases combining the SC physeal fracture [1, 4, 10, 14] or a true dislocation of the SC joint [8, 11] with an adjacent clavicle fracture.
Typically, these injuries occur in adolescent patients and during athletic activities, as in our patient. The exact mechanism for this association of lesions is unknown: it has been hypothesised [7, 11, 16] that the double lesion might be caused by sequential forces producing both injuries simultaneously. If the two lesions were caused by one force, sustaining one injury would have seemingly dissipated the energy necessary to cause the second lesion [16].
As our experience teaches, a correct and complete pre-operative evaluation (SC dislocations versus fractures; potential compromise of respiratory, neurovascular or other neighbouring structures) should be performed. Contrast CT imaging with three-dimensional reconstruction yields adequate information regarding neighbouring vasculature and alignment of the floating fragment [4, 5, 17], and is the modality of choice in an emergency setting. MRI, if available, and ultrasound imaging would in theory be ideal for the demonstration of articular and physeal anatomy and damage [5], and would have helped us in planning surgery better. Yet, direct surgical visualisation during open reduction provided similar information.
Non-operative treatment and closed reduction are not indicated, as the free fragment cannot be managed. Once excluded a true dislocation of the SC joint, treatment requires open reduction of the two fractures, fixation of the lateral fracture and suture of the torn periosteum at the physeal fracture. No further medial stabilisation is required, as the periosteal tube remains in its anatomic position and the attaching ligaments are intact to the periosteum [14].
As concerns the stabilisation of the lateral fracture, we recommend plate fixation, as reported in another case [1]. Tension band wiring, which has been reported in a case [4] should be condemned because of possible pin migration. As an alternative, sutures through drill holes in the bone have been proposed, which would circumvent the need for hardware removal [9, 10], yet this may require longer immobilisation.
References:
- Allen BF Jr, Zielinski CJ (1999) Posterior fracture through the sternoclavicular physis associated with a clavicle fracture: a case report and literature review. Am J Orthop 28(10):598–600
- Denham RH Jr, Dingley AF Jr (1967) Epiphyseal separation of the medial end of the clavicle. J Bone Joint Surg 49A:1179–1183
- Elliott AC (1986) Tripartite injury of the clavicle. S Afr Med J 70:115
- Falcone MO, Guinand R, Bachour F, Haidar N, Fontaine C, Chantelot C (2007) Bifocal fracture of sternal end of clavicle pseudodislocation of sternoclavicular joint. Report of a case. Chir Main 26(1):50–54
- Gobet R, Meuli M, Altermatt S, Jenni V, Willi UV (2004) Medial clavicular epiphysiolysis in children: the so-called sterno- clavicular dislocation. Emerg Radiol 10(5):252–255
- Goldfarb CA, Bassett GS, Sullivan S, Gordon JE (2001) Retro-sternal displacement after physeal fracture of the medial clavicle in children. J Bone Joint Surg Br 83B:1168–1172
- Hardy JRW (1992) Complex clavicular injury in childhood. J Bone Joint Surg 74B:154
- Kanoksikarin S, Wearne WM (1978) Fracture and retrosternal dislocation of the clavicle. Aust N Z J Surg 48(1):95–6
- Lehnert M, Maier B, Jacob H, Maier M, Laurer HL, Marzi I (2005) Fracture and retrosternal dislocation of the medial clavicle in a 12-year-old child case report, options for diagnosis, and treatment in children. J Pediatr Surg 40(11):e1–e3
- Lemire L, Rosman M (1984) Sternoclavicular epiphyseal separa- tion with adjacent clavicular fracture. J Pediatr Orthop 4(1):118– 120
- Nakazato T, Wada I, Tsuchiya D, Sugimura I, Tomita H, Matsui N (2001) Clavicle fracture and posterior sternoclavicular dislo- cation in a newborn. Orthopedics 24(12):1169–1170
- O’Neill PJ, Cosgarea AJ, McFarland EG (2000) Unusual double clavicle fracture in a lacrosse player. Clin J Sport Med 10(1): 69–71
- Pearsall AW 4th, Russell GV Jr (2000) Ipsilateral clavicle frac- ture, sternoclavicular joint subluxation, and long thoracic nerve injury: an unusual constellation of injuries sustained during wrestling. Am J Sports Med 28(6):904–908
- Rockwood CA, Wirth M (1996) Injuries to the sternoclavicular joint. In: Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds) Rockwood and green’s fractures in adults. 4th edn. Lippincott-Raven, Philadelphia, pp 1415–1471
- Tanlin Y (1996) Ipsilateral sternoclavicular joint dislocation and clavicle fracture. J Orthop Trauma 10(7):506–507
- Thomas CB, Friedman RJ (1989) Ipsilateral sternoclavicular dislocation and clavicle fracture. Case report. J Orthop Trauma 3:355–357
- Waters PM, Bae DS, Kadiyala RK (2003) Short-term outcomes after surgical treatment of traumatic posterior sternoclavicular fracture-dislocations in children and adolescents. J Pediatr Orthop 23(4):464–469










