Abstract
We report three cases of a broken locking mechanism of the acetabular components of Harris-Galante II cups. There was no trauma and none of the implants demonstrated evidence of loosening prior to failure. This complication after a total hip replacement is very rare, but may result in significant morbidity. All patients with this type of implant should be monitored for evidence of a locking mechanism constructed of polyethylene.
Résumé
Nous rapportons trois cas de rupture du mécanisme de verrouillage des cupules acétabulaires de Harris - Galante II. Il n'y avait aucun trauma et aucun des implants n'a montré des évidences de descellement. Cette complication aprčs une prothčse totale est trčs rare, mais il peut en résulter une morbidité considérable. Tous les malades avec ce type d'implant devraient ętre surveillés étroitement.
Introduction
Recently, studies have reported the excellent radiographic performance of porous-coated cementless acetabular components. No evidence of migration or loosening of the cups was reported, and only a very limited progression of radiolucent lines with short- and intermediate- term results was found [1,4,5]. Therefore, the success and the advantages of a modular component cementless total hip arthroplasty (THA) have become well known, and the use of acetabular components without cement for THA has increased dramatically in the last decade. However, some complications after cementless THA have also been reported [2,4,6]. The failure of the locking mechanism of acetabular components is very rare, but may result in severe complications [2]. Here, we describe 3 patients with broken locking mechanisms of acetabular components that underwent revision surgery.
Case report
Case 1
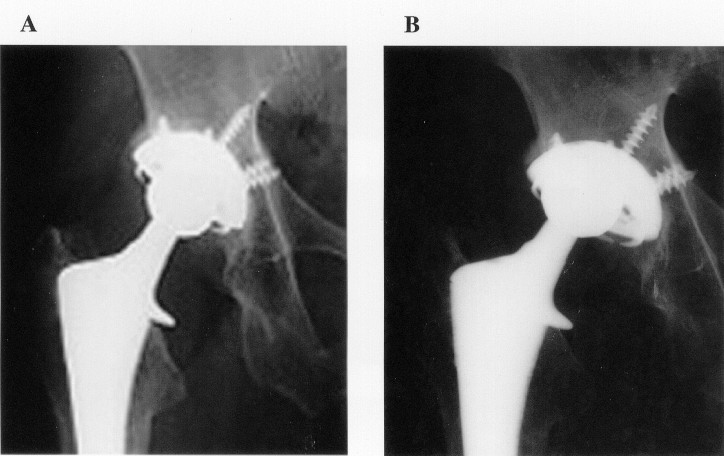
A 57-year-old man presented with an aseptic necrosis of the right femoral head, which resulted from steroid administration. In October 1992 he underwent a successful hip replacement using a Harris cementless femoral stem, a 26 mm cobalt-chrome femoral head, and a press-fit porous-coated Harris-Galante II 50-mm acetabular shell with polyethylene liner (Zimmer, Japan). Sixty-five months later he felt a sudden hip pain, and heard squeaking noises during motion of his right hip. The range of motion of the hip joint was limited by pain and radiographs showed an eccentric position of the femoral head within the acetabular component (Figure 1).
At revision surgery, a severe metallosis was present in the soft tissues and around the acetabular component. The outer acetabular shell was rigidly fixed by extensive ingrowth of bone. However, the four proximally located metal locking tabs were broken, and the polyethylene liner was dislocated from the outer shell. The metal stained soft tissue was removed, and the acetabular component was revised with a 52 mm press-fit trilogy acetabular shell and a 26-mm cobalt-chrome femoral head (Zimmer, Japan). The femoral stem component was not revised. Twenty-one months after the operation, the patient was free of pain and fully mobile.
Case 2
A 73-year-old woman with seronegative rheumatoid arthritis underwent a right hip replacement for severe arthritis using a press-fit porous-coated Harris-Galante II 48-mm acetabular shell with polyethylene liner, a 26 mm cobalt-chrome femoral head, and a Harris cementless femoral stem. After surgery, she was pain-free with good function. At follow-up, ninety months after primary surgery, she was not suffering any hip joint pain, and remained fully ambulatory. However, radiographs showed a clearly eccentric position of the head of the femoral prosthesis within the acetabular component.
At revision surgery, a moderate metallosis was present in the soft tissues and around the acetabular component. The polyethylene liner was dislocated from the outer shell, and four triangular metallic pieces were observed at the posterior portion of the shell (Figure 2). The outer shell was rigidly fixed to the base of acetabular bone. The metal stained soft tissue was removed, and the acetabulum was revised with a 50 mm press-fit trilogy acetabular shell, a 28 mm liner, and a 26-mm cobalt-chrome femoral head (Zimmer, Japan). The femoral component was not revised. At the sixteen months after the revision surgery, the recovery had been uneventful.
Case 3
A 62-year-old woman with secondary osteoarthritis of the left hip underwent a hip replacement using a press-fit porous-coated Harris-Galante II 52-mm acetabular shell with polyethylene liner, a 26 mm cobalt-chrome femoral head, and a Harris cementless femoral stem. After surgery, she was pain-free with good function. Thirty-eight months later she suddenly felt an incongruous sense of her left hip joint. And at this time, she did not feel any pain and was able to walk without a cane. The range of motion of the hip joint was not limited. A radiograph showed the femoral head clearly displaced in an eccentric position within the acetabular component, and four triangular metal locking tabs were observed at the distal end of the acetabular cup.
At revision surgery, a severe metallosis was present in the soft tissues and around the acetabular component. The polyethylene liner was dislocated from the outer shell, and the four triangular metal locking tabs were observed at the posterior portion of the shell. There was no loosening of the outer shell. The metal stained soft tissue was removed, and the acetabular cup was revised with a 52 mm press-fit trilogy acetabular component, a 28 mm liner, and a 26-mm cobalt-chrome femoral head (Zimmer, Japan). The femoral component was not revised. At the time of the most recent follow-up, at six months after the revision surgery, the recovery had been uneventful.
Discussion
Failure of the polyethylene liner-locking mechanism is a rare complication of the acetabular components in cementless THA [4,8]. Recently, however, reports of this complication have gradually increased. In our clinic, we have used Harris-Galante cups for the past 14 years, and the incidence of this complication is 1.3% (3/232). Misalignment of the acetabular component, misplacement of the liner, material fatigue, and overload of the cup (due to patients weight and/or physical labour etc.) are thought to result in the disassembly of the acetabular shell [3,6]. However, most of these previous reports do not associate the failure with these factors. In addition, the breakage of the metal fixation tab and the dissociation of the polyethylene liner in our cases also resulted in the absence of these factors (Case 1: weight 50kg, height 161 cm, sedentary worker; Case 2: weight 41 kg, height 152 cm, housewife, Case 3: weight 58 kg, height 154 cm).
The majority of this type of failure occurred in the Harris-Galante prosthesis [3, 6, 7]. Schmalzried reported that this weak fixation of the polyethylene rim in the tabs is due to the inadequate polyethylene locking mechanism, and that the locking mechanism should be improved [9]. The tab of the next generation acetabular component has been improved (trilogy cup). The broken locking mechanism of the acetabular component is very rare, but may result in significantly severe complications [2]. We recommended that all Harris-Galante hip prostheses that have used the prototype locking mechanism should be monitored with radiographs. Regular radiographs are essential because clinical symptoms are not always present and a delay in the recognition of failure may result in osteolysis, loosening, and metallosis.
When damage to the locking mechanism is suspected, an early revision of the shell should be performed instead of an exchange of the polyethylene liner, since the breakage of metal tabs may result in extensive metallosis and wear, cup dislocation, loosening, and osteolysis.
References
Legends
