SICOT e-Newsletter
Issue No. 56 - May 2013
Expert Corner
Surgical Management of Bankart OperationJacinto Monteiro & Marco Sarmento
Orthopaedic Department, University Hospital of Santa Maria, Academic Medical Centre - Lisbon, Portugal
Shoulder instability is a very common symptomatic problem and should be separated from minor or major instability related to laxity. Instability itself varies from patient to patient, regarding symptoms, and is affected by age and gender.
In patients less than 20 years of age the chance of recurrence is 60-70% and in patients older than 40 years it is less than 10%. Age is the main predictor factor in terms of recurrence.
Our criteria to propose a surgical treatment is related to the age of the patient, the number of episodes, direction, degree, aetiology of the dislocations, and the presence of structural lesions.
Bankart lesions, labral or osseus, are pathognomonic of traumatic instability of the shoulder, and when isolated, without any other structural lesion, have the best results with Bankart procedure.
We do not recommend routinely stabilising the young patient after the first episode of shoulder dislocation, unless we are in the presence of a high performance athlete or when the patient has persistent complaints of minor shoulder instability in his/her activities of daily life or in sports.
We do not consider proposing to operate a patient who voluntarily produces the instability.
Management:
After an adequate clinical evaluation supported by imaging exams (X-ray, TC, MRI or arthro-TC or arthro-MRI), we discuss with the patient what the proper procedure to solve his particular problem would be. It is very important to consider the functional expectations of the patient, the sporting activity performance expected, and the labrum/bone lesions presented.
The Bankart technique is the standard surgical procedure which we perform on our patients, and it accounts for about 90% of our surgical techniques for shoulder instability.
During the last 20 years we have performed the Bankart operation by an open technique using suture anchors to reattach the labrum with an average of 2/3 sutures per patient. Anterior capsular shifting was used in more than 80% of the patients as a complementary procedure.
In the last 4 years, we have been changing the Bankart technique to the arthroscopic approach. With arthroscopy, the large spectrum of lesions have been better recognised, mostly those from the posterior part of the shoulder. Also the quality of the repair became more accurate (localisation of the anchors and the amount of tissue mobilised and fixed) and this has resulted in a better recovery time and the same overall satisfactory outcome, with the same recurrence after repair.
Surgical Technique:
We do the Bankart arthroscopic procedure in the beach chair position with the arm to be operated in a free position. The beach chair position is our goal for all arthroscopic procedures, so it is routinely and easily set up by the operating room personnel. On the other hand, it helps the surgeon to be customised in spatial orientation, by doing all surgical approaches in the same manner.
During the last 20 years we have performed the Bankart operation by an open technique using suture anchors to reattach the labrum with an average of 2/3 sutures per patient. Anterior capsular shifting was used in more than 80% of the patients as a complementary procedure.
In the last 4 years, we have been changing the Bankart technique to the arthroscopic approach. With arthroscopy, the large spectrum of lesions have been better recognised, mostly those from the posterior part of the shoulder. Also the quality of the repair became more accurate (localisation of the anchors and the amount of tissue mobilised and fixed) and this has resulted in a better recovery time and the same overall satisfactory outcome, with the same recurrence after repair.
Surgical Technique:
We do the Bankart arthroscopic procedure in the beach chair position with the arm to be operated in a free position. The beach chair position is our goal for all arthroscopic procedures, so it is routinely and easily set up by the operating room personnel. On the other hand, it helps the surgeon to be customised in spatial orientation, by doing all surgical approaches in the same manner.
The surgery is performed routinely under general anaesthesia, which is normally associated with an interscalenic brachial plexus block to control pain in the first 24 hours post-op.
Portals:
We begin the arthroscopy by a posterior portal, and after the diagnostic tour of the inside of the shoulder, we complement the access by doing anterior and anterosuperior portals.
With a probe and changing the visual portal we finish our diagnostic part.
When there are only Bankart labral lesions, we try to mobilise the scarring labrum and stimulate the native bed of it. We start to fix with the most inferior part of the labrum and try to put the first anchor a little articular to the edge of the glenoid and the field is controlled with the scope in the anterosuperior portal. We use on average 2/3 anchors when an isolated Bankart lesion is present. Normally the first anchor is double loaded because it allows us to reattach the labrum in a wider position with the trickiest anchor placement.
In those cases where the Hill Sachs lesion has more than 25% of the size of the humeral head and when an external rotation and abduction motion of the upper limb put the lesion in an engagement position in the anterior glenoid rim, a remplissage is done. This infraspinatus tenodesis is performed firstly (before the labrum reattachment) in order to get more space in the posterior articular zone to achieve a better visualization.
In those patients doing high performance contact sports or with overhead demanding activities, and in those who had a huge number of dislocations with a bad quality or inexistent labrum, we convert the surgical procedure in an open Latarjet.
Post-operatively:
After the arthroscopic surgery the arm is suspended in a sling with a pillow between the arm and the chest to maintain the upper limb in a neutral position during 2 weeks.
The patient is allowed to be an outpatient the day after.
Between the 10th and the 15th day the stitches are removed.
The patient is taught to exercise the arm with pendular and circular exercises on the second day after the operation. The passive range of motion begins with physiotherapy supervision with external rotation limited to 10º and anterior flexion and abduction to 90º until 6 weeks. Active exercises and passive assisted exercises are then allowed over the initial limits.
Portals:
We begin the arthroscopy by a posterior portal, and after the diagnostic tour of the inside of the shoulder, we complement the access by doing anterior and anterosuperior portals.
With a probe and changing the visual portal we finish our diagnostic part.
When there are only Bankart labral lesions, we try to mobilise the scarring labrum and stimulate the native bed of it. We start to fix with the most inferior part of the labrum and try to put the first anchor a little articular to the edge of the glenoid and the field is controlled with the scope in the anterosuperior portal. We use on average 2/3 anchors when an isolated Bankart lesion is present. Normally the first anchor is double loaded because it allows us to reattach the labrum in a wider position with the trickiest anchor placement.
In those cases where the Hill Sachs lesion has more than 25% of the size of the humeral head and when an external rotation and abduction motion of the upper limb put the lesion in an engagement position in the anterior glenoid rim, a remplissage is done. This infraspinatus tenodesis is performed firstly (before the labrum reattachment) in order to get more space in the posterior articular zone to achieve a better visualization.
In those patients doing high performance contact sports or with overhead demanding activities, and in those who had a huge number of dislocations with a bad quality or inexistent labrum, we convert the surgical procedure in an open Latarjet.
Post-operatively:
After the arthroscopic surgery the arm is suspended in a sling with a pillow between the arm and the chest to maintain the upper limb in a neutral position during 2 weeks.
The patient is allowed to be an outpatient the day after.
Between the 10th and the 15th day the stitches are removed.
The patient is taught to exercise the arm with pendular and circular exercises on the second day after the operation. The passive range of motion begins with physiotherapy supervision with external rotation limited to 10º and anterior flexion and abduction to 90º until 6 weeks. Active exercises and passive assisted exercises are then allowed over the initial limits.
The return to full athletic activities is not recommended before the fourth month and this is extended to six months in contact sports (karate, rugby, judo).

Fig. 1: Metallic anchors position after open Bankart repair (AP view)

Fig. 2: Metallic anchors position after open Bankart repair (Axilar view)

Fig. 3: Typical acute shoulder dislocation (right arm)

Fig. 4: Patient in beach chair position for a Bankart arthroscopic procedure
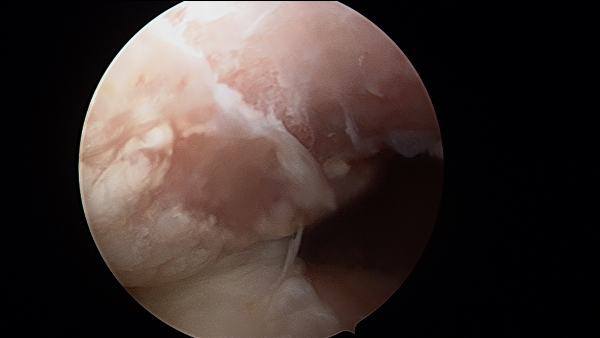
Fig. 5: Hill Sachs lesion in an anterosuperior view
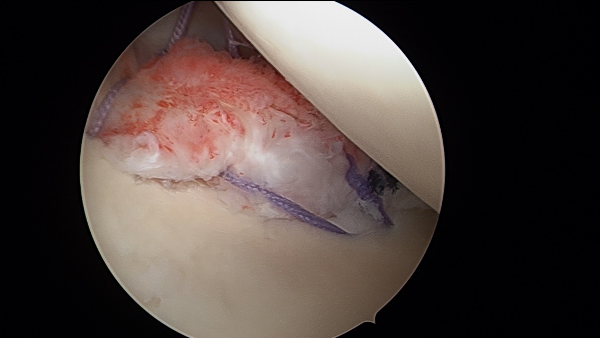
Fig. 6: Slight articular position of the most inferior double loaded anchor
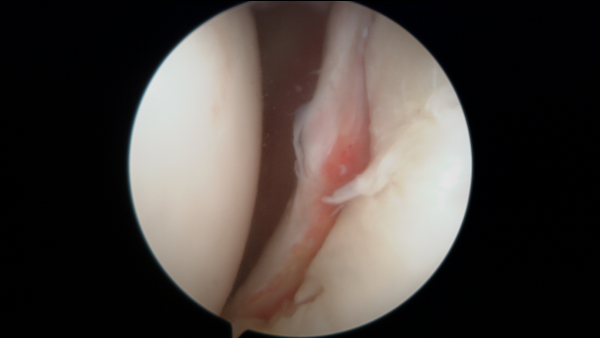
Fig. 7: Bankart lesion between the 2 and 6 oâclock positions in a left shoulder
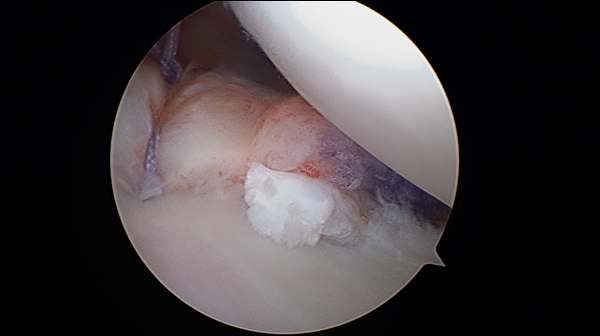
Fig. 8: Labrum reattachment and the fold created
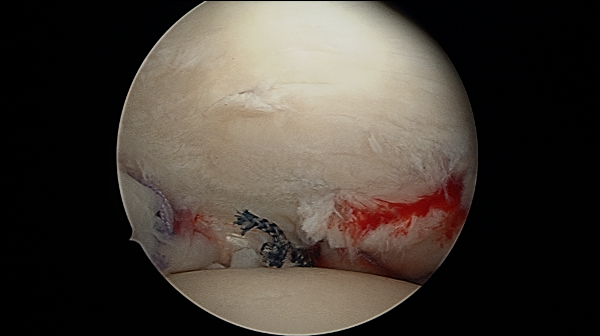
Fig. 9: Humeral head centered in the glenoid after the Bankart repair in an anterosuperior view
  Â